




A New Theoretical Perspective
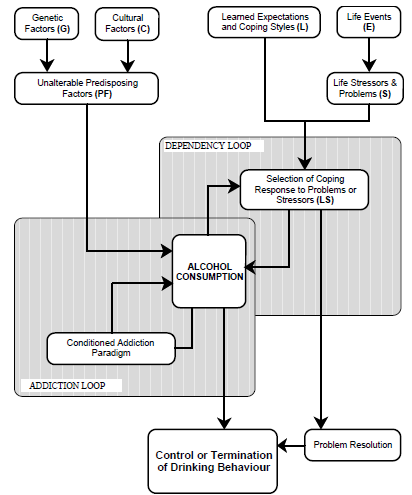
The schematic of this new and more inclusive theory is found in the accompanying diagram. It is a model that tries to explain the etymology of alcoholism using the current research available and suggesting hypotheses for further research. Like all models, this one will inevitably be modified over time, and perhaps ultimately discarded. Its main advantage is that it serves as a useful and effective tool to drive both research and treatment of the problem at hand: alcoholism.
The existence of Genetic Factors (abbreviated as the G-factor), which helps account for alcoholism rates, has long been recognized. Petrakis (1985), in his excellent survey of the research into the genetic factors contributing to alcoholism, makes this point obvious. Yet, genetic markers are not the sole determinant of whether a person will become an alcoholic. Petrakis points out that there are two types of genetic predispositions to alcoholism: milieu-limited and male-limited (1985:8). While the male-limited variety does seem to be unaffected by the post-natal environment, it accounts for less that 25% of all male alcoholics and around 4% of all general population males. This effectively accounts for less that 2% of the population. Milieu-limited alcoholism “is called milieu-limited because its occurrence and severity in susceptible offspring are influenced by the postnatal environment” (1985:8). Predispositions to alcoholism in females are attributed to this milieu-limited model. Unlike the heavy drinking male-limited alcoholic, milieu-limited alcoholism is characterized by mild to moderate alcohol abuse and as such, may not even be assessed as alcoholism by experts.
The fact that the postnatal environment affects the occurrence of this second type of alcoholism suggests that genetic markers alone are not sufficient predictors of alcoholism occurrence in an individual. For this reason, Cultural Factors (or C-factor) and learned expectations are also important. This importance is perhaps most salient in discussing the difference between Jellinek's concepts of gamma and delta alcoholism (1960:38). Gamma alcoholism is found in North America and is characterized, among other things, by a loss of control but not necessarily an inability to abstain. Delta alcoholism common to Europe is characterized by an inability to abstain but seldom involves a loss of personal control over one’s drinking. The cultural influences affecting drinking behaviour and thus alcoholism rates can be found not only in cross-cultural studies, but also in intra-cultural research (Gusfield, 1962; Lawrence and Maxwell, 1962; Bales, 1962). It is proposed that these cultural factors mediate the rate of alcoholism in three ways: first, they determine the level of acceptable exposure to alcohol and therefore the quantity, frequency and regularity of alcohol consumption. Second, cultural factors affect the general attitudes which members of the culture, or social class have towards alcohol consumption. In this way, the relative approval or disapproval of alcohol use is culturally determined. In the same way, the culture has much to do in influencing individuals to look upon alcohol consumption in a positive or negative light. Finally, cultural factors as more broadly represented in the way political and economic forces determine the price of alcohol and thus, influence alcohol consumption (Popham and Schmidt, 1962:26).
Both these factors, genetic markers and cultural influences, serve as Unalterable Predisposing Factors (called the PF-factor) in the development of alcoholism. These predisposing factors are important elements in determining the potential of the person to become an alcoholic. In this way they may well be necessary elements in the development of alcoholism in an individual, and while it is possible that they may be sufficient factors in some cases, such as male-limited alcoholism, they are usually only contributing factors in the development of alcoholism. They are called “Unalterable” because they are given factors and are not easily altered by therapeutic interference or preventative counseling. It is possible that some people may become alcoholic simply because of their G-factors, C-factors or combined PFfactors, but the experiences of many alcoholics cannot be accounted for simply by reference to PF-factors. Other factors need to be investigated and accounted for in the overall attempt to explain alcoholism.
Learned Expectations and Coping Styles (or L-factor) are similar to cultural factors except that they refer to the specific values and expectations found in the family of origin and the individual's peer group and can therefore be quite distinct from the cultural values of the society as a whole (Boothroyd, 1980). These expectations affect drinking behaviour in a number of different ways. The perceived effects of alcohol consumption and whether these effects are seen in a positive or negative light have been found to display a strong correlation with eventual alcoholism.
Presumably, these attitudes to alcohol are acquired from the family of origin and play a major part in determining how the individual will come to evaluate alcohol consumption and whether or not the person will use or abuse alcohol or abstain altogether (Christiansen and Brown, 1985; Christiansen, Goldman and Brown, 1985; Christiansen and Goldman, 1983). It is argued that if people come to see alcohol in a positive light and feel that alcohol improves social behaviour, increases arousal, and decreases tension, they will be more likely to use alcohol in an attempt to achieve these ends (Christiansen, Goldman and Brown, 1985). Similarly, they will be more likely to turn to alcohol to enhance recreational enjoyment as well as coping with life stress and anxiety and, it is hypothesized, they are more likely to abuse alcohol and become alcoholics.
Learned expectations concerning alcohol also affect alcohol consumption directly by teaching the individual when it is appropriate to consume alcohol. Furthermore, these expectations affect alcohol consumption indirectly by providing the individual with a set of coping or problem solving strategies to use in resolving Life Stressors and Problems (or the S-factor). The interaction of these life stressors and the person's coping abilities leads to a Selection of Coping Response to Problems or Stressors, called the LS-factor, and plays an important role in whether the person will drink, and why. If this repertoire of strategies is too narrow or lacks effectiveness, or if the repertoire suggests an acceptability in using drugs or alcohol in order to relieve tension or stress, then it is more probable that the individual will turn to drug and alcohol use to cope with life stress and anxiety and perhaps become an alcoholic. For example, a young man whose father, whenever under life stress came home to beat the mother, has just recently moved in with a new girlfriend himself. Having learned a coping strategy from his own father, namely wife beating, as a way of dealing with stress, he comes to respond in kind. To alleviate the guilt that emerges from this ineffective strategy, he may well turn to alcohol. In this way, alcoholism becomes a secondary product of the learned responses acquired from the family of origin.
From the schematic, we can see that individuals consume alcohol for a combination of two reasons: as part of the coping strategy in response to life stressors, and for purely social, cultural and hence recreational purposes. The interaction of these two components, the PF-factor and the LS-factor, will determine if the person's drinking is explained as a response either to predisposing factors, or life stressors, or some combination of the two. It is more able to account for reasons why a person drinks, and is better suited to looking for the causes, and consequently the remedies of drinking.
This model also accounts for why some people can voluntarily control their own excessive drinking without external assistance. If their drinking is in response to life stressors and they have not developed into an addiction or dependency, they have a great deal of control over their decision to drink. If the life stressor contributing to the problem is resolved, the incentive to drink is lessened. As well, the person may decide on their own to control or terminate their drinking behaviour.
The person becomes an alcoholic only when they become physically addicted, psychologically dependent or both addicted and dependent to alcohol. The Dependency Loop demonstrates how alcohol use can become its own problem. By turning to alcohol consumption as a problem solving strategy, the reasons for the stress are not dealt with and will usually build up thus generating even more stress and psychic tension, which must be relieved, once again by turning to alcohol. In addition, behaviour while intoxicated, such as assault, breaking furniture or drunken driving can add its own problems to the total S-factor. If alcohol consumption is personally viewed in a positive light and if it becomes a prime coping strategy, then there is a high probability that the individual will become psychologically dependent on alcohol.
It must be cautioned that psychological dependency infers much more than a lack of “will-power”. A person is psychologically dependent not because they lack the personal discipline to control their drinking, but because the psychological “payoffs” in drinking far outweigh the “debts”. With such a high degree of payoffs to drinking, will power has very little to do with a person's dependency on alcohol. Of course, there may come a time when the debts outweigh the payoffs. At this point, the person may either stop drinking if they have not become addicted to alcohol, or else continue to drink in order to avoid the physical debts of addiction which will ensue should consumption be stopped.
The Addiction Loop represents both a pharmacological response and a classically (or Pavlovian) conditioned response to alcohol consumption. More research needs to be done before the actual nature of physical addiction is understood and as this research becomes available, it is probable that the exposition of the Addiction Loop may be significantly modified. Current research is suggesting that what has traditionally been called pharmacological addiction is better understood by using a Pavlovian conditioning paradigm.
As Hinson and Siegel (1983), Kesner and Raymond (1983) have discovered in studying the effects of morphine addiction, regular and conscious drug usage instills an unconscious expectation in the individual for future drug usage. In anticipation of continued regular and persistent drug use, the body attempts to counteract the expected effects of the drug by enhancing the body's reaction to the drug's effects and in this way, rapidly returns the animal's physiology to a state of equilibrium. For example, if the animal has come to expect regular doses of morphine, a drug that is both a sedative and an anesthetic, the body compensates for the expected effects of morphine injections by increasing the animal's level of hyperactivity and sensitivity to pain. If by past experience, the drug comes to be expected on a regular and predictable schedule and the drug is not forthcoming, the physiology will still respond in anticipation of the drug and the animal will be overly hyperactive and sensitive. In effect, the body will be out of equilibrium because the expected drug was not forthcoming. Support for this view with particular reference to alcohol studies shows that if an alcoholic is given alcoholic beverages to consume but is told they are not receiving any alcohol, they do not exhibit a loss of control (Marlatt and Rohsenow, 1980).
Clearly, the imbalance or “debt” which we call addiction is psychological and conscious in origin although it does manifest both psychological and physical distress if the expected chemical is not forthcoming. This distress is called “withdrawal”. Because there is a strong desire by the individual to return to the expected equilibrium, he person will develop a strong craving for the drug in order to return their physiology to a normal state or in other words, to avoid withdrawal. The role of expectations regarding drinking behaviour explains why a conditioned addiction to alcohol is often present in the chronic alcoholic (Milam and Ketcham, 1985). It is easily seen that, contrary to the disease model understanding that sees alcoholism as a maladaptive and destructive response, an addiction approach sees the development of alcoholism as a natural and healthy bodily response to the persistent introduction of a noxious substance. Like acquiring a suntan in the continued presence of ultraviolet radiation, the body’s ability to respond to the presence of alcohol is an adaptive rather than maladaptive one. If the body were unable to respond, the imbiber would soon die, just as the sun-tanner would soon shrivel up with skin cancer. It is these two loops, the addiction loop and the dependency loop which separate alcoholism from the non-alcoholic drinker. It is recognized that an alcoholic can be either dependent or addicted to alcohol or even both dependent and addicted simultaneously. However, more often than not, a person progresses from a psychological dependency to a physical addiction. This switch from dependency to addiction accounts for the development or stages of alcoholism that the disease theorists describe (Milam & Ketcham).